Explaining the Brain: The Brain Stem
When the Engine Room Fails: Understanding Brainstem Injury

Moshi, is a retired engineer, and he was a master of detail, from complex engineering blueprints to the tasting notes in his wife’s precise cardamom tea recipe.
One morning, his world literally tilted. He reached for his tea and the kitchen slid sideways. Not a brief dizzy spell. Not the kind that passes in a few seconds if you hold still. The floor pitched like the deck of a boat. The ceiling fell and the floor rose. He grabbed the table edge and it didn’t help, because the problem wasn’t gravity, it was his inner world on a tilt, his brain. While he remained awake and cognitively himself; He knew his name, knew his daughter’s name, knew exactly what was happening and how frightening it was, he couldn’t change it, his body had stopped obeying. He could not stand without falling. He could not walk a straight line. The vestibular system in his brain that had done its job for 72 years had simply, without warning, stopped reporting accurately.
He was diagnosed with a lateral medullary infarct, a stroke in the lowest part of his brainstem.
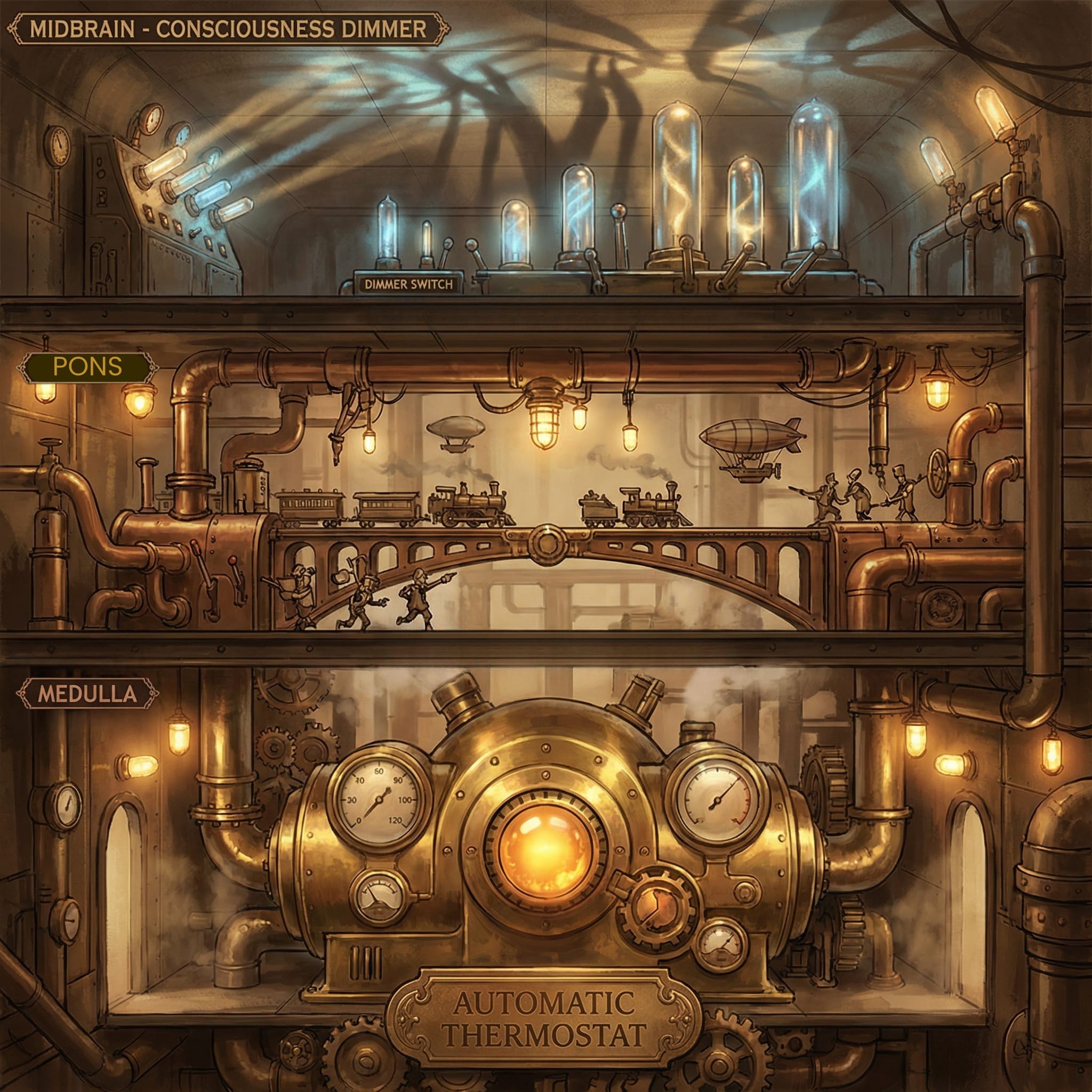
To understand Moshi’s injury, perhaps we should think like him. Picture the brain as a high-rise office building:
The Cortex (The CEO): The top floors where strategy, memory, and personality live. Moshi’s CEO was perfectly fine.
The Brainstem (The Engine Room): The basement containing the engine, electrical grid, plumbing, and ventilation.
If the ventilation fails, it doesn’t matter how brilliant the CEO is; the building becomes uninhabitable. The brainstem is what biologists call: Highly Conserved, meaning it is so essential for life that its design has remained nearly identical across millions of years of evolution.
The Three Floors of the Engine Room
1. The Medulla: The Automatic Thermostat
Bottom: The medulla is the lowest section, connecting the brain to the spinal cord. It manages “set-it-and-forget-it” functions like heart rate, blood pressure, and the complex rhythm of breathing.
The “Crossed Wire” Mystery (Wallenberg Syndrome): Moshi experienced a strange phenomenon, the left side of his face felt numb, and the right side of his body lost sensation. Think of the brain’s sensory wires like cables in a wall. The body’s cables cross over to the opposite side further down in the spinal cord, but the face’s cables stay cross over at the medulla. A single hit to the side of the medulla catches the body cables that already crossed and the face cables that haven’t yet, creating a seemingly opposite sided reaction in the face and body.
2. The Pons: The Grand Central Bridge
Middle: The word Pons is Latin for “bridge”. It acts as a massive relay station for signals traveling between the CEO above and the Project Manager (the cerebellum) behind it. It also houses the sleep switch that regulates REM sleep. Moshi’s pons was spared but had his stroke drifted even slightly upward, the bridge that kept his eyes moving, his face feeling, and his nights restful might have failed him too.
3. The Midbrain: The Consciousness Dimmer Switch
Top: The midbrain is the top floor of the brainstem. It houses the Ascending Reticular Activating System (ARAS). Think of the ARAS as a dimmer switch for consciousness. If this switch is damaged, the “lights” of the cortex cannot turn on, leading to coma or altered consciousness. It also contains the substantia nigra, which produces dopamine. Damage here can cause Parkinson-like stiffness and slow movement, and because the face loses its expressiveness, it’s often mistaken for depression by families and clinicians alike.
Clinical Application
For PT/OT: Moshi’s experience is a “gyroscope” problem in the medulla. Use gaze stabilization and be wary of hidden sensory loss, he may not feel a hot cup with his right hand or the left part of his lips.
For RN/NPs: Aspiration pneumonia is the primary threat. Because Moshi’s “CEO” is awake and talking, it’s easy to forget his “Plumbing” (swallowing reflex) is broken.
For Mental Health: Moshi is cognitively intact. He understands exactly what he has lost, and that clarity is its own kind of suffering. There is a particular psychological weight that comes with this presentation. Moshi doesn’t have the protective fog of confusion or memory loss. He remembers who he was last Tuesday. He remembers what his hands could do, what his voice sounded like, what it felt like to walk across a room without falling. He is grieving in real time, with full awareness, every single day of his recovery. Rehabilitation counselors call this the “adjustment to disability” process, a nonlinear, deeply personal reckoning with the gap between a person’s pre-injury identity and their current functional reality. For Moshi, that gap includes his role as a grandfather, a tea-connoisseur, a detail oriented engineer, a husband, a man who prided himself on his independence. These aren’t small losses. They are identity losses. And identity loss, left unaddressed, predicts poor rehabilitation outcomes. The brain doesn’t wait for the healing process. It runs at full speed, cataloguing every deficit, every limitation, every moment of dependence, and without support, that process curdles into helplessness, withdrawal, and treatment refusal.
Depression following brainstem stroke is common and underdiagnosed, in part because (as noted above) the flat affect of midbrain involvement can mask it, and in part because clinicians are busy managing the medical acuity. But the research is clear: Untreated depression after acquired brain injury significantly reduces functional recovery and community reintegration.

Today, Moshi is currently in rehabilitation therapy with an OT, relearning to swallow. His “engine room” is slowly repairing itself, and the unique tasting notes in his wife’s tea are waiting for him at home.
For the complete version of these free neuroanatomy courses, including free handouts for your clinic, clients, and their family members; Connections between lessons; The Invisibility Gap identifying social justice aspects; The Technical Bit inclusions for explicit anatomical detail; and For the Clinicians sections for differential diagnosis and clinical decision-making, subscribe to our email list to receive these mini-lessons to your inbox: https://www.braininjurytherapy.org/explainingthebrainregister